High Blood Pressure is just another term for hypertension. When the heart beats and pumps blood through the body, it exerts a certain amount of force against blood vessels. We can check our blood pressure at home or the doctor’s office by using an arm cuff. There are two parts of a blood pressure reading while measuring; these are:
- Systolic pressure (the top number)
- Diastolic pressure (the bottom number)
This article will provide necessary information about hypertension. How we can keep it in check to live a long and healthy life without worrying about blood pressure getting out of control again.
Defining Hypertension:
We can define hypertension as persistently high pressure exerted by blood in systemic arteries. Blood pressure measures the ratio between systolic blood pressure (SBP) and diastolic blood pressure (DBP).
The following are the definitions of systolic and diastolic blood pressure:
Systolic Blood Pressure (SBP): Systolic blood pressure refers to the pressure produced by blood on the walls of arteries as the heart contracts, and blood is forced out of its chambers.
Diastolic Blood Pressure (DBP): The pressure exerted by blood on the walls of arteries when the heart relaxes between heartbeats and refills with blood is called diastolic blood pressure.
Usually, systolic blood pressure equal to or above 140 millimetres of mercury (mmHg) and diastolic blood pressure similar to or above 90 millimetres of mercury (mmHg) is considered an indicator for hypertension.
According to the hydraulic equation, blood pressure is directly proportional to the product of blood flow (cardiac output) and resistance faced by blood when passing through arteries (perivascular resistance). Blood pressure is controlled by regulating these factors in normal and hypertensive patients.
Hypertension is also known as a “silent killer,” as most hypertensive people are unaware that they are hypertension because there are no significant signs and symptoms. According to WHO data, there are more than 1 billion cases worldwide of hypertension with the age range between 30-79 years. Most of the cases are from low-income and middle-income countries. Approximately 46% of these patients are unaware that they have hypertension. Hypertension is also a significant cause of premature deaths worldwide.
Hypertension Basics & types:
Typically blood pressure is represented by a hydraulic equation in which blood pressure is in direct proportion to the product of cardiac output (CO) and peripheral vascular resistance (PVR)
BP = CO x PVR
The above equation shows that an increase or decrease in blood pressure is directly related to cardiac output and peripheral vascular resistance. Hence increase in any or both of these values tends to increase blood pressure.
Usually, blood pressure regulation in our body is regulated by
- Cardiac Output
- PVR (usually occurs at arterioles, postcapillary venules, and heart)
- Kidneys (maintain the fluid balance of our body)
Above these are then controlled by the collective effect of
- Baroreflexes which are mediated by autonomic nerves
- Renin-Angiotensin-Aldosterone System (RAAS) in Kidneys
- Local vasoactive substances (endothelin-I and Nitric Oxide).
Primary / Essential Hypertension:
Studies show that patients with essential hypertension do not have one cause. However, it is a combination of abnormalities in factors controlling and maintaining blood pressure in our body (baroreflexes, RAAS). Of all the patients diagnosed as hypertensive, almost 95% of them have primary essential hypertension in which there is increased blood pressure due to multiple genetic and environmental factors. These patients do not have an underlying disease or condition due to which their blood pressure elevates. There is elevated blood pressure due to increased peripheral vascular resistance (PVR) in most cases. However, there is no increase in cardiac output.
- These abnormalities may be due to
- Genetic factors (heredity causes up to 30%, genetic mutations)
- Poor lifestyle
- Psychological stress
- Salts imbalance( increase sodium intake, decrease potassium and calcium intake)
Secondary Hypertension:
It is a type of hypertension that occurs due to the disease. 5% of patients have hypertension due to any disease or syndrome. Secondary hypertension usually occurs early due to any genetic disease or old age. It can also be seen in those patients whose first diagnosis is essential hypertension and are receiving more than three antihypertensives and are showing now or slight reduction in blood pressure.
Causes of secondary hypertension usually are:
- Genetic causes (Liddle syndrome, Gordon Syndrome)
- Sleep apnea
- Drug-induced or drug-related
- Chronic kidney disease
- Primary aldosteronism
- Renovascular disease
- Long-term corticosteroid therapy and Cushing syndrome
- Pheochromocytoma
- Thyroid or parathyroid disease
How to diagnose hypertension?
Usually, multiple readings are recorded to diagnose hypertension. According to American Heart Association (AHA), diagnosis can not be made on a single elevated blood pressure reading unless the reading is above 180/110 mmHg with the presence of any heart disease.
Multiple readings and doctor’s office visits are required to diagnose blood pressure, usually with 1-4 weeks intervals.
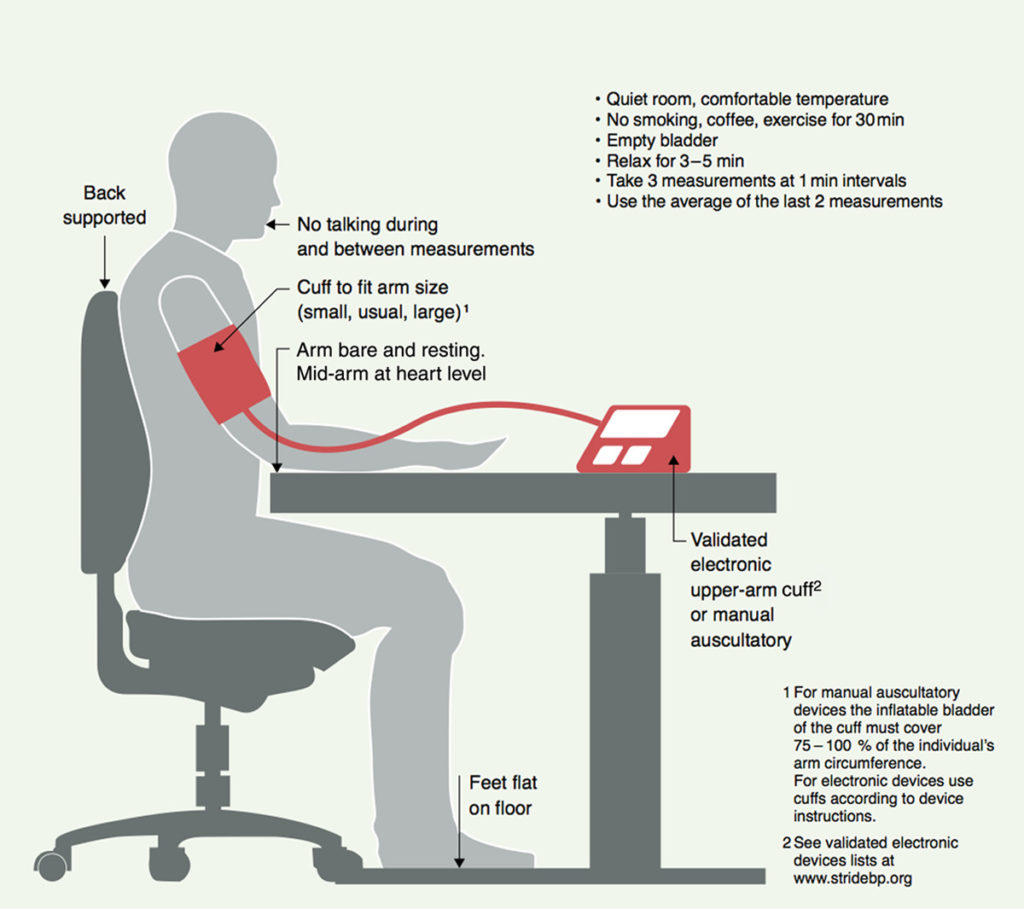
Techniques to measure blood pressure:
To measure blood pressure following procedure is followed:
- The patient must be sitting in a relaxed way and comfortable position.
- The patient should be sitting supine for at least 5 minutes or 30 minutes after smoking or having coffee.
- Use of appropriate size cuff.
- Blood Pressure is checked with calibrated manual or automated device
- Blood pressure is measured in both arms.
- If there is a difference of 15mmHg in one arm, that arm is used for further readings.
- Blood pressure should be checked both in sitting and standing positions to identify changes in blood pressure due to changes in posture.
Multiple approaches and methods of blood pressure measuring are used to confirm the diagnosis of hypertension. Methods include:
- Office blood pressure monitoring
- Home blood pressure monitoring
- Ambulatory Blood pressure Monitoring
Blood pressure readings obtained outside the doctor’s office, either by the patient at home or by an automated device set to record readings at periodic intervals (ambulatory blood pressure), are more robust predictors of results and are suggested in clinical recommendations.
The patient’s blood pressure elevates in a hospital or clinical setting and is normal in the home.
Home measurement of blood pressure also helps identify White Coat hypertension, which is treatment-resistant. It also helps identify Masked Hypertension in which blood pressure readings are recorded normally in a hospital or clinical setting but are high when outside the hospital or clinic.
Categorisation of Hypertension:
As per National Institute of Health and Care Excellence (NICE) guidelines, blood pressure can be categorised.
| Clinic blood pressure | ABPM daytime average or HBPM average blood pressure | |
| Stage 1 hypertension | 140/90 mmHg to 159/99 mmHg | 135/85 mmHg to 149/94 mmHg |
| Stage 2 hypertension | 160/100 mmHg to 180/120 mmHg | 150/95 mmHg or higher |
| Stage 3 or severe hypertension | 180 mmHg or higher systolic blood pressure or diastolic blood pressure recorded in the clinic is 120 mmHg or higher. |
Complications Associated with Hypertension?
Consistently elevated blood pressure leads to severe complications and organ damage in the body. Not being able to diagnose on time increases the risk of complications more than on-time diagnosis. Following are the lists of complications associated with hypertension:
- Heart or CV complications (these complications are the most common in hypertensive patients and are the primary cause of morbidity and mortality related to patients in hypertension)
- Left ventricular hypertrophy
- Angina or prior myocardial infarction
- Prior coronary revascularisation
- Heart failure
- Brain
- Stroke or transient ischemic attack
- Chronic kidney disease
- Peripheral arterial disease
- Retinopathy
Treatment of Hypertension:
Hypertension is a chronic condition that cannot be treated, but it can be controlled well by using different treatment methods which are developed by years of research and clinical trials
Treatment options include:
Treatment without medicines (Non-Pharmacologic): Non Pharmacologic treatment involves a lifestyle modification approach. This method is mainly used for patients with essential hypertension. As essential hypertension is primarily due to environmental factors, these factors focus on controlling hypertension. Non-Pharmacologic approach involves
- Weight loss: Reduces in systolic blood pressure of 0.5–2 mmHg per kg weight loss can be observed in overweight persons.

Smoking cessation: Although smoking has no direct influence on blood pressure, it does raise cardiovascular risk. Therefore, patients should quit smoking or minimise it if that is not possible.
- Reduce alcohol intake: Limit consumption to 2 drinks/day in men and one drink/day in women and lighter-weight persons
Diet control: In clinical research, the Dietary Approaches to Stop Hypertension (DASH) diet reduced blood pressure markedly (4.5/2.7 mmHg) compared to a regular US diet. This diet emphasises vegetables, low-fat dairy products, fish, low-fat chicken, and whole grains while lessening red meat, sweets, and sugary beverages.
- Physical activity: Regular exercise should be encouraged, with a weekly goal of 150 minutes of moderate-intensity exercise or 75 minutes of high-intensity training. Physical activity leads to an increase in physical health and a decrease in blood pressure.
- Reduction in salt intake: Patients should limit their salt consumption by not adding salt to food during cooking, instead of utilising spices to improve flavour, and not adding salt to food on the plate. The goal should be to consume fewer than 100 mmol of sodium per day (equivalent to 6 g sodium chloride or 2.4 g elemental sodium).
Processed meat, ready meals, cheese, and even bread contain a significant quantity of concealed salt. A nutritional evaluation may be necessary to precisely evaluate a patient’s salt intake and suggest reducing it.
Treatment with medicines (pharmacological treatment): Lifestyle changes are generally the primary management option for low-risk stage 1 hypertension. However, if drug treatment is more urgently required, such as stage 2 and severe hypertension, lifestyle modifications must start with drug therapy.
Pharmacological treatment involves the use of oral antihypertensive agents. Following is the list of oral antihypertensive drugs used to treat hypertension.
| Drug Class | Drug Name |
| Angiotensin converting enzyme inhibitor (ACEi) | Ramipril Lisinopril Perindopril Enalapril |
| Angiotensin receptor blockers (ARBs) | Candesartan Irbesartan Losartan Valsartan |
| Calcium channel Blocker (CCB) | Amlodipine Felodipine Lacidipine Lercanidipine Diltiazem Verapamil |
| Diuretics | Indapamide Chlortalidone Bendroflumethiazide Hydrochlorothiazide Furosemide Bumetanide |
| Aldosterone antagonists | Spironolactone Eplerenone |
| Beta-blockers | Bisoprolol Atenolol Metoprolol Nebivolol Labetalol |
| α-Blockers | Doxazosin Prazosin |
| Centrally acting vasodilator | Methyldopa Moxonidine |
High blood pressure, or hypertension, refers to any consistent reading of 140/90 mmHg or above. If you have hypertension, it’s essential to seek treatment as soon as possible because even slight elevations in blood pressure can lead to serious health issues such as heart disease and stroke. Because hypertension generally has no symptoms, most people aren’t aware they have it until it’s too late.
High blood pressure, or hypertension, can be severe, even fatal, if untreated. But it’s easy to avoid and control once you know what to look out for and how to take care of it by following established guidelines.